Colorectal or colon cancer is among the top three cancers for both men and women in South Africa with 1 in 77 males and 1 in 132 females diagnosed according to the National Cancer Register (2019). There is evidence of many younger individuals being diagnosed with colorectal cancer.
It’s the second most common cancer in men (following prostate cancer) and the third most common cancer in women (following breast and cervical cancer).
Regular Screening & early detection can not just save your life, but also reduce the risk of needing a colostomy pouch.
Did You Know?
- Colorectal cancer in its early stages shows no symptoms. It is often diagnosed late when at a more advanced stage or it has spread to other parts of the body.
- It is therefore important to be aware of family history and to take advantage of screening for colorectal cancer before symptoms are experienced, and not to wait until experiencing discomfort.
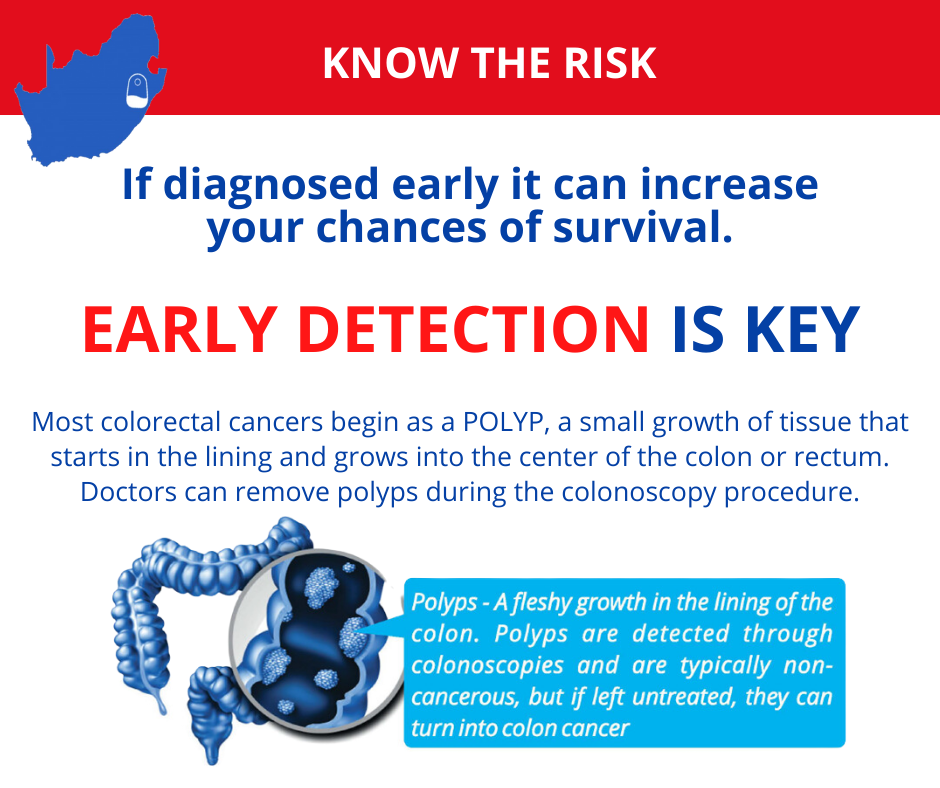
- Most colorectal cancers begin as a polyp, a small growth of tissue that starts in the lining & grows into the centre of the colon or rectum. Doctors can remove polyps during the colonoscopy procedure.
- Treatment depends on how far the cancer has advanced and may include surgery, radiation, chemotherapy, or a combination of these therapies.
People with symptoms or signs that suggest the presence of colorectal cancer or polyps should be offered the appropriate diagnostic evaluation.
Screening programmes should begin by classifying the individual patients level of risk based on personal, family and medical history, which will determine the appropriate approach to screening in that person.
Men and women at average risk should be offered screening for colorectal cancer from age 50.
They should be offered options for screening after being given information about the advantages and disadvantages of each method, and should be given an opportunity to apply their own preference in selecting how they should be screened.
An abnormal screening test must be followed by a complete examination of the colon, preferably by colonoscopy (or flexible sigmoidoscopy and double contrast barium enema if colonoscopy is not available.)
Individuals at increased risk should be by means of colonoscopy. This group includes: Those with previous colorectal cancer
- History of prior adenomatous polyps
- Patients with an underlying condition which predisposes to colorectal cancer e.g. inflammatory bowel disease
Health care providers performing these tests should have appropriate proficiency, and the tests should be performed correctly. Standards and operating procedures should be set.
Screening must be accompanied by efforts to optimise the participation of patients and health care providers, both in the initial screening and in the rescreening at recommended intervals.
Screening Average Risk Individuals
- Faecal Occult Blood Testing
Yearly or biennial faecal occult blood testing (FOBT) has been shown to reduce colorectal cancer mortality by 21%. Drawbacks of this method of screening include low compliance rates, high false positive rates leading to colonoscopy with its associated cost, discomfort and complications, and high false negative rates. Depending on the type of test used patients may require dietary restriction such as avoiding red meat. This may further reduce compliance.
The finding of a positive faecal occult blood test should result in a colonoscopy being performed, as this examination is superior in accuracy to double contrast barium enema. - Flexible Sigmoidoscopy
Sigmoidoscopy performed every 5 years has been shown to reduce colorectal cancer deaths by up to two thirds for lesions within reach of the sigmoidoscope. Cancer risk above this level was not reduced. Repeat screening every 5 years has been shown to be optimal. This is less than the interval for colonoscopy, and reflects the lower sensitivity of sigmoidoscopy, from examining less of the colon, but also a less thorough examination as bowel preparation is often sub-optimal, varied experience of examiners, and the effect of patient discomfort limiting the depth of insertion of the sigmoidoscope.
Having found an adenoma on sigmoidoscopy, the decision to proceed to colonoscopy should be individualized. Studies have shown that positive sigmoidoscopy followed by colonoscopy would detect 70-80% of advanced proximal neoplasia, and reduce cancer incidence by 80%. - Combined FOBT and Flexible Sigmoidoscopy
Annual FOBT and 5 yearly sigmoidoscopy is yet another method of screening for colorectal cancer. This approach has now been studied in a randomised control trial. Sigmoidoscopy detected 70% of patients with advanced neoplasia, and the addition of a one-time FOBT increased the rate to 76%. Another study showed a significant additional yield by adding sigmoidoscopy to FOBT testing. Three times as many cancers and 5 times as many large adenomatous polyps were identified in the combined group. When this method of screening is used, the FOBT must be done first, as a positive FOBT is an indication for colonoscopy.
The disadvantages of this approach are the additional costs, inconvenience and complications of both tests with an uncertain gain in effectiveness. - Colonoscopy
Colonoscopy is able to detect lesions in both distal and proximal colon, and one has the possibility of removing polyps found at this examination. An interval of 10 years between examinations after a negative colonoscopy is recommended. This is based on the finding that the dwell time from the development of adenomatous polyps to transformation to cancer is estimated to be at least 10 years on average. Fewer than 6% of clinically important adenomas are missed at colonoscopy. Recent studies have confirmed that 50% to 65% of patients with advanced proximal neoplasia had no distal colonic neoplasms.
The costs, inconvenience and complications need to be considered in advising colonoscopy as a screening method. Colonoscopy may not be widely available, and expertise in performing the examination varies widely. - Double-Contrast Barium Enema
Double-contrast barium enema (DCBE) offered every 5 years has been used for colorectal cancer screening. DCBE has lower sensitivity than colonoscopy for detecting cancers and large polyps, and the examination does not permit removal of polyps, or biopsy of cancers. False positive examinations may occur due to presence of stool. An abnormal DCBE must be followed by colonoscopy.
DCBE is offered because of lower cost, examination of the whole colon, wide availability, and detection of about half of large polyps. The combination of DCBE and sigmoidoscopy is not recommended for screening.
In a surveillance population DCBE detected 53% of adenomatous polyps 6-10mm in size, and 48% of adenomas >1cm in size.

Discussion
The “average risk” of colorectal cancer in the western world is estimated at 6%. Screening strategies have been shown to prevent the risk of colorectal cancer. The challenge is to communicate this knowledge to the wider public, to health care providers and funders, and then to complete the screening process.
Colorectal cancer screening is more complex than screening for breast and cervical cancer, where one type of test is required (mammography, Pap smear).
For screening to be successful doctors must remember to offer screening, patients must accept this advice, insurers must pay for screening and follow-up testing, and patient-care organisations must have systems to track whether screening has taken place and to give reminders if it has not.
Advanced colorectal cancer is a devastating disease, and is preventable with appropriate screening methods. It is with this in mind that the South African Gastroenterology Society (SAGES) and its allied professional groups, is embarking on a colorectal cancer prevention campaign. The aim is to reach the health care professionals, the public at risk and the funders to heighten awareness, and to stimulate action. The initiative will culminate during the South African Digestive Diseases Week (SADDW) in August 2003.
The source of this article is largely from the American Society of Gastroenterology Guideline published in Gastroenterology in February 2003.
Dr H.R.Schneider
(SOURCE: https://www.sages.co.za/Professional/SagesStatements06)
Risk Factors
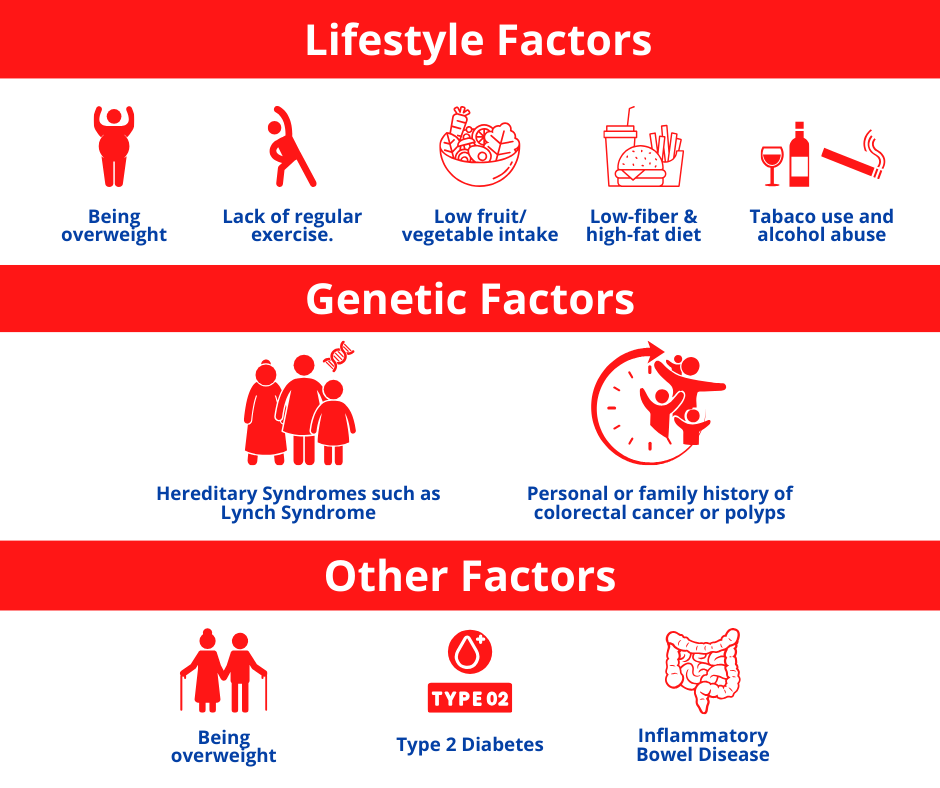
Lifestyle factors such as lack of regular exercise; low fruit / vegetable intake; low fibre and high fat diet; obesity; alcohol abuse; tobacco use and poor oral hygiene. Hereditary syndromes (Lynch Syndrome); a personal or family history of polyps or colorectal cancer; inflammatory bowel disease; type 2 Diabetes and old age are other risk factors.
Symptoms
In early stages symptoms are not present, however when they do occur, they may include:
- change in bowel habits (diarrhoea / constipation / consistency of stools)
- rectal bleeding or blood in stools
- persistent abdominal discomfort (cramps, gas or pain not related to diet)
- a feeling that the bowel does not completely empty
- weakness or fatigue
- unexplained weight loss
Need Support?
CANSA offers professional pre- and post-operative counselling and support groups at our Stoma Clinics and Stoma bags and linen savers can be purchased at reduced prices at most local CANSA Care Centres. CANSA provides stock of the biggest stoma brands and guarantees the lowest prices, professional assistance and speedy delivery.
The CANSA Tele Stoma Support Service offers online consultations for stoma patients and their families to assist with challenges or stoma queries. Make an appoinment on 0800 22 66 22.